

Thoracic Outlet Syndrome
Have you ever felt pain, numbness, or tingling in your neck, shoulder, or arm? If so, you may be experiencing thoracic outlet syndrome (TOS). Don't worry; we will cover all the essential information about this condition, which affects the nerves and blood vessels in your upper chest and neck.
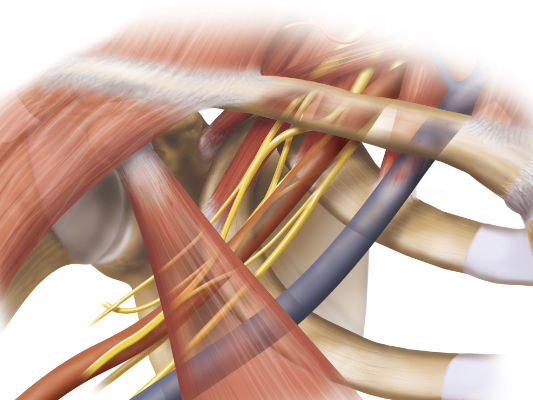
Thoracic outlet syndrome occurs when nerves or blood vessels are compressed, causing sensory symptoms or blood flow abnormalities in either or both upper extremities. This compression results from anatomical abnormalities or repetitive movements. Doctors classify TOS into three types: neurogenic TOS, venous TOS, and arterial TOS. Neurogenic TOS involves the brachial plexus, a network of nerves that controls movement and sensation in the arm.
Common causes of TOS include compression by the anterior scalene muscle, a cervical rib (an extra rib located above the normal first rib), trauma, or repetitive motions in non-ergonomic positions, such as when using a computer at work. There is no need to memorize everything right now; we'll delve deeper into these concepts together soon.
Let's get started!

Table of Contents
Symptoms of Thoracic Outlet Syndrome
Thoracic outlet syndrome (TOS) is a condition that can cause a range of symptoms, often affecting the neck, shoulder, and arm. It is essential to recognize these symptoms to seek proper diagnosis and treatment. Here are some common signs to watch out for:
- Pain in the neck, shoulder, and arm: One of the most prevalent symptoms of TOS is pain in these areas. The pain may be sharp or dull and can vary in intensity. It may radiate down the arm or into the fingers. Individuals with TOS often experience discomfort that worsens with specific activities such as lifting heavy objects, raising the arms overhead, or repetitive motions.
- Numbness and tingling sensations: Another telltale sign of thoracic outlet syndrome is numbness and tingling in the affected areas. This sensation can occur in the neck, shoulder, arm, hand, or fingers. It may feel like pins and needles or a loss of sensation altogether. These sensations can be persistent or intermittent.
- Weakness or muscle wasting: In advanced cases of TOS, individuals may notice weakness or muscle wasting, specifically in their hands. These muscle changes result from severe and long-standing compression of nerves that control hand movements. As a result, tasks requiring fine motor skills, such as writing or gripping objects tightly, may become challenging.

While these symptoms are commonly associated with thoracic outlet syndrome, they can also indicate other conditions. Patients should always consult with a healthcare professional for an accurate diagnosis. In addition to these symptoms of TOS, several other factors suggest the presence of thoracic outlet syndrome:
- Similar symptoms occur in other conditions: Some individuals with TOS may experience symptoms similar to those seen in carpal tunnel syndrome or cervical radiculopathy (a pinched nerve in the neck). These symptoms include wrist pain, grip strength weakness, and pain radiating down the arm.
- Signs of vascular involvement: In some instances, TOS can affect blood vessels, leading to swelling, discoloration, or coldness in the affected arm. You should seek prompt medical attention if you notice any of these signs with other TOS symptoms.
Causes and Risk Factors for Thoracic Outlet Syndrome
Thoracic Outlet Syndrome (TOS) results from several overlapping factors. Knowledge of the causes and risk factors associated with TOS allows a patient to seek an earlier diagnosis and early intervention. Let's delve into some of the key contributors to this condition.
Anatomical Abnormalities
One common cause of TOS is anatomic abnormalities in the thoracic outlet region. These abnormalities can compress nerves and blood vessels in the area, resulting in symptoms of TOS. Anatomic abnormalities include extra ribs (cervical ribs), additional or variant muscles, and fibrous bands in the neck, shoulder, or upper chest. Such abnormalities cause TOS by exerting pressure on vital structures.
Repetitive Movements and Poor Posture
Repetitive movements involving the arms and shoulders can increase the risk of developing TOS. Activities such as typing, carrying heavy loads, or participating in sports that require frequent overhead motions may strain the muscles and soft tissues around the thoracic outlet. Prolonged slouching posture or hunching over a desk while working can also lead to muscle imbalances and compression within this region.
Occupational Risks
Certain occupations pose a higher risk for developing TOS due to their repetitive nature or specific demands on the upper body. Jobs that involve constant overhead reaching, such as painters, electricians, or athletes involved in throwing sports like baseball or swimming, may find themselves at greater risk for developing TOS. Over time, these activities place repetitive or continuous stress on the thoracic outlet structures.
Pregnancy
Some authorities believe that pregnancy can also be a contributing factor to TOS. As a woman's body changes during pregnancy, hormonal fluctuations may lead to increased laxity in ligaments and joints, weight gain, and swelling. These changes can contribute to the compression of nerves and blood vessels within the thoracic outlet region.
Trauma and Injuries
Trauma or injuries to the neck or shoulder area can trigger the onset of thoracic outlet syndrome (TOS). Accidents, such as car collisions or falls, can cause immediate and direct damage to the structures in the thoracic outlet, leading to compression of nerves or blood vessels and subsequent symptoms.
Genetic Predisposition
While rare, there may be a genetic component to TOS. Some individuals may have an inherited predisposition for anatomical abnormalities or connective tissue disorders that increase their susceptibility to developing this condition, such as Ehlers-Danlos syndrome.
Understanding the causes and risk factors associated with thoracic outlet syndrome is essential for prevention and early intervention. Knowing these potential triggers can allow individuals to take proactive steps to reduce their risk and seek appropriate treatment.
Diagnostic Tests for Thoracic Outlet Syndrome
TOS specialists rely on specific provocative tests to help diagnose TOS. During a typical physical exam, a doctor evaluates a patient's posture, range of motion, and muscle strength in the affected areas. However, experienced TOS specialists also perform specific maneuvers known as provocative tests to reproduce symptoms and determine if they are consistent with thoracic outlet syndrome.
Imaging tests like X-rays, MRI scans, or CT scans can help identify any structural abnormalities contributing to TOS. X-rays provide a basic view of the bones in the neck and shoulder region, allowing doctors to rule out other conditions that may mimic TOS symptoms. Magnetic resonance imaging (MRI) uses powerful magnets and radio waves to create detailed images of soft tissues such as muscles and nerves. These images can help detect any compression or abnormalities in the affected area. Similarly, computed tomography (CT) scans provide cross-sectional images that allow for a more precise evaluation of structures within the thoracic outlet than X-rays.
Electromyography (EMG) and nerve conduction studies (NCS) are often applied to assess nerve function in suspected cases of TOS. These tests involve using small electrodes placed on the skin that measure electrical activity produced by underlying muscles and nerves. EMG helps determine the presence of muscle weakness or damage due to nerve compression, while NCS evaluates how well the involved nerves conduct electrical signals. However, many authorities believe that EMG/NCS does not detect TOS until late in the course of the disease.
In addition to these specific diagnostic tests, a comprehensive medical history review is crucial for accurate diagnosis. A doctor will ask about specific TOS symptoms, their frequency and intensity, and any previous injuries or activities that might have contributed to the development of TOS. Experienced TOS specialists often ask detailed questions about the evolution of symptoms over time and during a typical day, as well as the positions or activities that exacerbate or relieve symptoms.
During the physical examination, a doctor may perform provocative tests such as Adson's maneuver or Roos' test. Adson's maneuver involves checking for changes in pulse at the wrist while rotating the patient's head towards the affected side and taking a deep breath. A doctor performs Roos' test by holding both arms with elbows bent and hands overhead and repeatedly opening and closing the hands. A positive Roos' test reproduces symptoms such as numbness or tingling.
It is important to note that the diagnosis of thoracic outlet syndrome can be challenging due to its complex nature. The symptoms often overlap with other conditions, making it essential for healthcare providers to perform a thorough evaluation using a combination of physical examination, imaging tests, and nerve function assessments. By employing these diagnostic tools, doctors can accurately diagnose TOS and develop an appropriate treatment plan tailored to each individual's needs.
Treatment Options for Thoracic Outlet Syndrome
Treatment options include surgical and non-surgical (or conservative) options. Non-surgical or conservative treatment for TOS includes physical therapy exercises designed to calm the nervous system, alleviate the compression on the nerves and blood vessels in the thoracic outlet area, retrain breathing, stretch muscles, and improve posture. Physical therapy can be highly effective in reducing pain and improving functionality for individuals with TOS.
Some of the common thoracic outlet syndrome exercises include:
- Calm the nervous system: In people with chronic pain, the central nervous system (the brain and spinal cord) often becomes hypersensitive to normal, non-painful stimuli. When this change is present, relief of compression of peripheral nerves may not accomplish enough reduction of perceived pain.
- Alleviate compression of nerves and blood vessels: Compression of nerves or blood vessels as they pass through the thoracic outlet typically creates the necessary elements for thoracic outlet syndrome. In many cases, physical therapy can alter the positions of the chest, neck, shoulder blades, and collarbones, reducing or eliminating this pressure and halting damage to the nerves and blood vessels.
- Retrain breathing: Breathing requires complex coordination of airways, chest wall structures, and respiratory muscles. Patients with TOS often develop abnormal or dysfunctional breathing, such as underutilizing primary respiratory muscles and relying overly on secondary respiratory muscles, including the scalene muscles. Retraining breathing may allow the scalene muscles to relax, reducing compression of nerves and blood vessels in the thoracic outlet.
- Stretching: Stretching exercises improve flexibility and reduce muscle tension in the affected area. Stretching can reduce or alleviate compression on the nerves and blood vessels. Examples of stretching exercises include shoulder rolls, neck stretches, and pectoral stretches.
- Improve posture: As TOS patients suffer pain in the neck and upper extremities, they reposition their neck, head, and shoulders to ease this pain. These new and abnormal neck and shoulder postures can change the body's center of gravity, forcing the patient to compensate by changing the posture of their hips, pelvis, and lumbar spine. These changes can lead to lower back and hip pain and alter breathing mechanics. A physical therapist knowledgeable in TOS can recognize these changes and help the patient regain normal and functional posture.
Some physical therapists recommend strengthening exercises to build up the muscles of the thoracic outlet to provide better support and stability. However, many physical therapists who treat TOS patients caution against strengthening exercises until all other issues are adequately resolved. Even then, TOS patients should use caution when beginning strength training, as they may suffer rapid setbacks. These strengthening exercises typically target the shoulder girdle, upper back, and neck muscles. Some examples of strengthening exercises include scapular retractions, rows, and shoulder shrugs.
In addition to physical therapy, pain medication or anti-inflammatory drugs may be prescribed to manage symptoms associated with thoracic outlet syndrome. These medications can help reduce pain, inflammation, and swelling. It is essential to follow your healthcare provider's instructions regarding dosage and frequency when taking these medications.
In some cases, doctors may perform injections into the muscles and around the nerves of the thoracic outlet. These injections may contain corticosteroids, anesthetic agents such as lidocaine, muscle relaxants such as Botox, and biologic agents such as platelet-rich plasma. When targeted towards specific thoracic outlet structures, these agents can have powerful anti-inflammatory or muscle-relaxing properties that temporarily relieve TOS symptoms.
While non-surgical or conservative treatments are often successful in managing thoracic outlet syndrome, there may be instances where surgical treatment is necessary. Doctors consider surgery when conservative treatment has failed to provide adequate relief or if there is significant nerve damage present.
Surgical options for treating thoracic outlet syndrome vary depending on individual cases but may include:
- First rib resection: Compression of nerves and blood vessels frequently occurs between the collarbone and the first rib in TOS patients. Removal of the first rib typically relieves pressure on the nerves and blood vessels in the thoracic outlet.
- Scalene muscle release or resection: In this surgical procedure, the scalene muscles that may be compressing the nerves and blood vessels are detached or removed.
- Vascular repair surgery: If there is significant arterial or venous compression, damage to these blood vessels may result in an arterial aneurysm or venous blood clot. Along with the above surgeries to reduce compression of the blood vessel, repair of the damaged segment of the affected blood vessel is typically indicated.
It is essential to consult with a healthcare professional to determine the most suitable treatment approach for your specific condition. They will consider factors such as the severity of your symptoms, underlying causes, and overall health before recommending an appropriate treatment plan for thoracic outlet syndrome.
Surgical Procedures for Thoracic Outlet Syndrome
If non-surgical treatments fail to provide relief from the symptoms of thoracic outlet syndrome (TOS), many patients consider surgical intervention, typically called thoracic outlet decompression surgery. This procedure aims to alleviate the compression of nerves and blood vessels in the affected area by removing any structures causing the obstruction.
During thoracic outlet decompression surgery, a skilled surgeon carefully identifies and eliminates all sources of compression. The specific surgical procedures for TOS can vary depending on the individual circumstances of each TOS patient. Still, they generally involve removing a portion of a rib, removing tight muscles, or performing both to relieve compression. Let's delve into these procedures in more detail.
Rib Resection
One common surgical approach for thoracic outlet syndrome involves removing a portion of the first rib. This procedure helps create additional space within the thoracic outlet region, relieving pressure on compressed nerves and blood vessels. The surgeon makes an incision along the side of the neck to access the affected area. They then remove a section of the first rib responsible for causing compression.
If the patient has a cervical rib, the surgeon may target the cervical rib instead of the first rib or may remove both.
Doctors can perform rib resection through several different approaches, including:
- Supraclavicular approach: The surgeon makes an incision above the collarbone to reach the thoracic outlet. This approach allows the surgeon to see the scalene muscles and brachial plexus clearly and to dissect the soft tissues around the brachial plexus. The surgeon can remove a good portion of the lateral part of the first rib but may not be able to remove all of the anterior and posterior portions of this rib.
- Transaxillary approach: With the patient's arm held above the head in a support mechanism, the surgeon makes an incision in the axilla (armpit). This approach allows the surgeon to see the lateral part of the first rib but does not allow resection of the anterior or posterior parts of this rib. This approach also allows the surgeon to see the brachial plexus and blood vessels as they pass over the first rib, which enables resection of the insertions of the anterior and middle scalene muscles on the first rib. Resection of a cervical rib can prove difficult through this approach.
- Infraclavicular approach: The surgeon makes an incision underneath the collarbone to reach the most anterior part of the first rib. Some TOS surgeons consider this an optimal approach to decompress the subclavian vein, but some TOS surgeons also use this approach to treat neurogenic thoracic outlet syndrome.
- Paraclavicular approach: The surgeon makes two incisions, one above and one below the clavicle. This approach is optimal in some patients who suffer from both neurogenic TOS and venous TOS.
- Video-Assisted Thoracoscopic Surgery (VATS): This minimally invasive technique utilizes small incisions, specialized tools such as fiberoptic cameras, and video guidance to perform rib resection.
- Robotic surgery: Using advanced robotic assistance devices, specially trained surgeons can approach the thoracic outlet from unique angles and perform surgical techniques that would otherwise be impossible.
Muscle Resection and Release
Decompression of the thoracic outlet often requires more than just a rib resection. During a typical first rib resection, the surgeon frequently removes or resects soft tissues compressing nerves or blood vessels in the thoracic outlet. The surgeon may resect all or parts of the anterior scalene muscle, middle scalene muscle, and accessory muscles such as a scalene minimus muscle. If the surgeon finds a fibrous band, they will resect it. By carefully dissecting and dividing these constricting muscles, surgeons aim to relieve pressure on vital structures.
Muscle release procedures may involve addressing various muscles that commonly contribute to compression, including:
- Scalene Muscles: The scalene muscles in the neck and upper chest can become tight and compress the nerves and blood vessels.
- Pectoralis Minor Muscle: This muscle, situated beneath the pectoralis major muscle, can also contribute to thoracic outlet compression when excessively tight.
- Subclavius Muscle: Located beneath the collarbone, the subclavius muscle can compress structures passing through the thoracic outlet.
By surgically releasing these muscles, surgeons aim to restore proper function and alleviate symptoms associated with thoracic outlet syndrome.
Surgeons call resection of a portion of the anterior scalene muscle 'anterior scalenectomy.' You might have heard a similar term, 'anterior scalenotomy.' This term refers to a simple release of one end of the anterior scalene muscle by cutting the insertion of that muscle on the first rib. Theoretically, this should reduce tension on the anterior scalene muscle and free up space in the thoracic outlet. Alfred Adson of the Mayo Clinic performed this procedure on TOS patients with cervical ribs in the 1920s. Several of his patients suffered a recurrence of symptoms, and the procedure fell out of favor.
Management and Physical Therapy for Thoracic Outlet Syndrome
Physical therapy is an essential component of managing thoracic outlet syndrome (TOS). It focuses on calming the nervous system, reducing compression of nerves and blood vessels, improving posture, restoring healthy breathing patterns, and increasing flexibility to alleviate pain and improve overall function. By combining techniques such as manual therapy, stretching exercises, and postural education, physical therapists help individuals with TOS regain control over their daily activities.
One of the primary goals of physical therapy for TOS is to provide pain relief. Manual therapy techniques, including soft tissue mobilization and joint manipulation, can help reduce muscle tension and alleviate discomfort. These hands-on approaches target specific areas affected by TOS, promoting relaxation and improved blood flow to the affected regions.
Stretching exercises often play a crucial role in relieving pain associated with TOS. Physical therapists guide patients through different stretches that target the muscles surrounding the thoracic outlet and the muscles that determine the positions of the shoulders. These stretches aim to increase flexibility, reduce muscle tightness, and improve overall range of motion. By incorporating these exercises into their daily routines, individuals with TOS can experience significant relief from pain.
In addition to manual therapy and stretching exercises, postural education is a vital aspect of physical therapy for TOS management. Physical therapists assess an individual's posture during various activities, such as sitting at a desk or lifting objects. They then provide guidance on proper body mechanics to minimize strain on the upper body. Ergonomic modifications at workstations can reduce stress on the thoracic outlet structures while performing job-related tasks.
Modifying daily activities is another key component of managing TOS through physical therapy. Individuals learn to avoid repetitive movements that may exacerbate symptoms or place additional strain on the affected areas. Patients can make simple adjustments like taking breaks during prolonged computer use or using ergonomic tools to reduce TOS symptoms or prevent recurrence.
People with TOS should work closely with their healthcare team, including doctors of different specialties and physical therapists. These team members can provide personalized care plans tailored to the individual's specific needs. By following their recommendations and actively participating in physical therapy sessions, individuals can experience improved health outcomes and better manage their TOS symptoms.
Outlook and Prognosis for Thoracic Outlet Syndrome
In conclusion, patients and their healthcare team can improve the outlook and prognosis for thoracic outlet syndrome if they understand the disease and the value of each treatment modality. While each case is unique, there is good reason for hope for improvement and relief from the symptoms of TOS. Each patient can take proactive steps toward recovery by identifying the causes, undergoing diagnostic tests, and exploring treatment options such as physical therapy or surgery.
Remember, your journey to recovery may require patience and persistence. TOS patients do better when they work closely with their healthcare team to develop a personalized treatment plan that suits their needs. With proper management and a commitment to therapeutic exercises, patients can significantly reduce pain, restore function, and improve their quality of life.
Thoracic Outlet Syndrome FAQs
What are the common risk factors for thoracic outlet syndrome?
Some common risk factors for thoracic outlet syndrome include repetitive arm motions (such as those performed by athletes or musicians), poor posture, trauma (such as car accidents or falls), pregnancy, anatomical abnormalities (such as extra ribs), and specific occupations that involve heavy lifting, prolonged overhead activities, or extensive time spent at non-ergonomic workspaces.
Can thoracic outlet syndrome be cured without surgery?
In many cases, TOS patients can effectively manage their disease and regain function without surgery. Non-surgical treatment options, such as physical therapy exercises focused on stretching muscles around the shoulder girdle area, can help alleviate symptoms and improve overall function. However, surgical intervention may be necessary in those cases where conservative measures fail to provide relief or nerve damage is present.
How long does it take to recover from thoracic outlet syndrome?
The duration of recovery from thoracic outlet syndrome varies depending on several factors, including the severity of the condition, individual response to treatment, adherence to rehabilitation protocols, and overall health status. Some individuals experience significant improvement within a few weeks or months with conservative treatments like physical therapy, while others may require a more extended period before experiencing relief.
Can I continue my regular activities while managing thoracic outlet syndrome?
Most TOS patients need to modify or avoid activities that exacerbate their symptoms during the management of thoracic outlet syndrome. However, with proper guidance from healthcare professionals, patients can gradually reintroduce activities into their routine as the condition improves. It is crucial to strike a balance between staying active and avoiding overuse or strain on the affected area.
Are there any long-term complications associated with thoracic outlet syndrome?
If left untreated or poorly managed, thoracic outlet syndrome can lead to potential complications such as chronic pain, muscle weakness, muscle atrophy (wasting), and nerve damage. It is essential to seek out experienced TOS specialists and to follow recommended treatment plans to minimize the risk of these long-term complications.


